Last reviewed: March 2026
Contents
MDM Templates
BRUE — Low Risk
Infant presents with a brief, resolved episode of color change, breathing irregularity, and tone change, now returned to baseline. Event lasted less than one minute. No CPR required by a trained medical provider. This is the first such event.
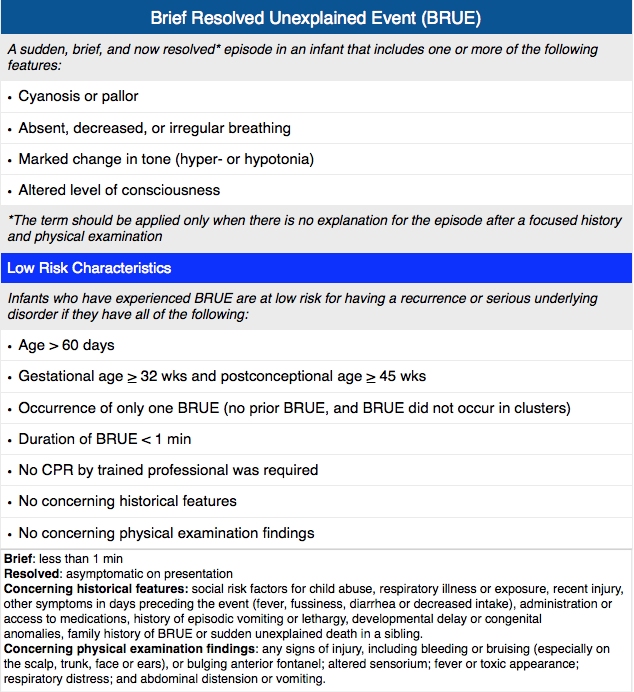
Low-risk criteria met per AAP 2016 guidelines: age >60 days, born ≥32 weeks with corrected gestational age ≥45 weeks, first event, duration <1 minute, no CPR by trained provider, and no concerning features on history or exam.[1]
Well appearing with normal vital signs and non-focal exam. No features concerning for seizure, cardiac arrhythmia, sepsis, foreign body aspiration, GERD, or non-accidental trauma.
Plan: Observed in ED for >1 hour without recurrence. Family educated that BRUE is not associated with SIDS and carries an excellent prognosis. Discharge with PCP follow-up within 24-48 hours. Return precautions for recurrence, color change, breathing difficulty, poor feeding, or lethargy.
Optional studies per AAP for low-risk BRUE: pertussis testing (NP swab), 12-lead ECG, brief pulse oximetry monitoring. Labs and imaging not recommended.[1]
BRUE — Higher Risk
Infant presents with a brief, resolved event as above but does not meet all low-risk criteria — specifically: ***.
Given higher-risk classification, expanded evaluation and observation warranted per AAP 2016 guidelines. Workup guided by clinical concern.[1]
Plan: Admit for cardiorespiratory monitoring. Consider ECG, glucose, pertussis testing, and additional studies based on clinical suspicion. Further workup and disposition determined by clinical course and results.
Clinical Education
What is a BRUE?
BRUE replaced the old term ALTE (Apparent Life-Threatening Event) in 2016. The AAP deliberately retired ALTE because it was overly broad, led to excessive testing, and included events that were never actually life-threatening.[1]
A BRUE must involve ≥1 of the following in an infant <1 year: cyanosis or pallor (not acrocyanosis), absent/decreased/irregular breathing, marked change in tone (hyper- or hypotonia), altered level of responsiveness.[1]
Critical distinction: The event must be brief, resolved by the time of evaluation, and unexplained after a thorough history and physical. If an explanation is found (seizure, GERD episode, UTI), it is NOT a BRUE — it is the underlying diagnosis, and management follows that diagnosis.
Risk Stratification
The entire purpose of the AAP 2016 guideline is risk stratification. Low-risk infants can be safely discharged with minimal testing. Higher-risk infants need individualized evaluation.[1]
| Criterion | Low Risk (ALL must be met) |
| Age | >60 days |
| Gestational age | ≥32 weeks AND corrected GA ≥45 weeks |
| Prior events | First event (no prior BRUEs) |
| Duration | <1 minute |
| CPR | No CPR required by trained medical provider |
| H&P | No concerning features on history or exam |
If ANY single criterion is not met, the infant is higher risk and requires individualized evaluation beyond the low-risk pathway.
Low-Risk Workup: Less is More
The AAP explicitly recommends AGAINST routine labs, imaging, or admission for low-risk BRUE. The entire point of the low-risk classification is to reduce unnecessary testing and hospitalization.[1]
What you CAN do (optional, shared decision-making): pertussis testing (NP swab), 12-lead ECG, brief pulse oximetry monitoring in the ED.
What you should NOT do for low-risk BRUE: CBC, BMP, blood cultures, CXR, CT head, EEG, echocardiography, UGI series — unless there is specific clinical suspicion directing the workup.
Observe ≥1 hour in the ED, educate the family, and discharge with close follow-up.
What BRUE is NOT
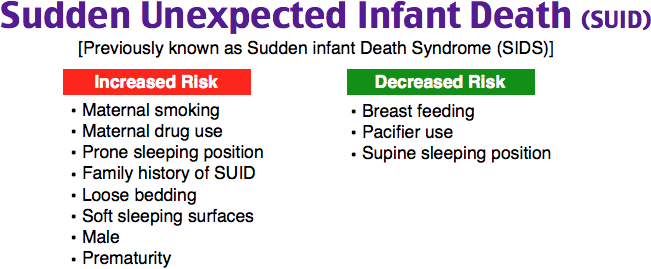
BRUE is NOT associated with SIDS. This is the single most important point for family counseling. Parents are terrified their child is going to die — reassure them that the data shows no association between BRUE and SIDS.[2]
Periodic breathing is NOT a BRUE. Normal brief respiratory pauses (<20 seconds) without desaturation or color change are expected in young infants.
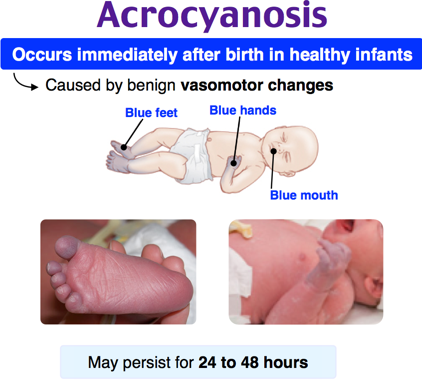
Acrocyanosis is NOT a BRUE. Blue hands and feet with a warm pink trunk is a normal finding in neonates — it is peripheral and does not indicate hypoxia or a concerning event.
Also NOT BRUEs: choking or gagging during feeds (often normal), breath-holding spells (have a clear precipitant — crying, pain, startle), and events with a clear explanation found on H&P (these are the underlying diagnosis, not a BRUE).
When to Worry — Higher-Risk Features
Age <60 days is the biggest risk factor — especially <30 days, where the differential broadens to include sepsis, meningitis, cardiac arrhythmia, and NAT. Consider a more extensive workup in very young infants.[1]
Other higher-risk features: prematurity, multiple events in 24 hours, event duration >1 minute, CPR required by trained provider, concerning social history (consider NAT), abnormal exam findings, and history suggestive of seizure, ingestion, or abuse.
These patients need individualized workup — there is no standardized protocol for higher-risk BRUE. Workup should be guided by clinical suspicion (ECG if arrhythmia concern, glucose and electrolytes if metabolic concern, head CT if NAT concern, etc.).
Disposition and Family Counseling
Low-risk: Discharge after ≥1 hour ED observation without recurrence. PCP follow-up within 24-48 hours. Safe sleep counseling (back to sleep, firm surface, no co-sleeping, no soft bedding). Offer infant CPR resources — many families want to feel empowered after a frightening event.[3]
Higher-risk: Admit for cardiorespiratory monitoring. Duration of monitoring depends on clinical course and workup results. Subspecialty consultation as indicated.
The most important counseling point: BRUE is not SIDS. These events are frightening for families but carry an excellent prognosis in the low-risk group. Validate their fear, provide clear return precautions, and ensure close follow-up.
References
- Tieder JS, Bonkowsky JL, Etzel RA, et al. Brief resolved unexplained events (formerly apparent life-threatening events) and evaluation of lower-risk infants. Pediatrics. 2016;137(5):e20160590. PubMed
- Brand DA, Altman RL, Purtill K, et al. Yield of diagnostic testing in infants who have had an apparent life-threatening event. Pediatrics. 2005;115(4):885-893. PubMed
- Moon RY; Task Force on Sudden Infant Death Syndrome. SIDS and other sleep-related infant deaths: evidence base for 2016 updated recommendations for a safe infant sleeping environment. Pediatrics. 2016;138(5):e20162940. PubMed
