Last reviewed: March 2026
Contents
MDM Templates
Isopropyl Alcohol Ingestion
Patient presents altered after suspected isopropyl alcohol ingestion. Airway intact, protecting airway. Fruity/acetone odor on breath. No focal neurologic deficits.
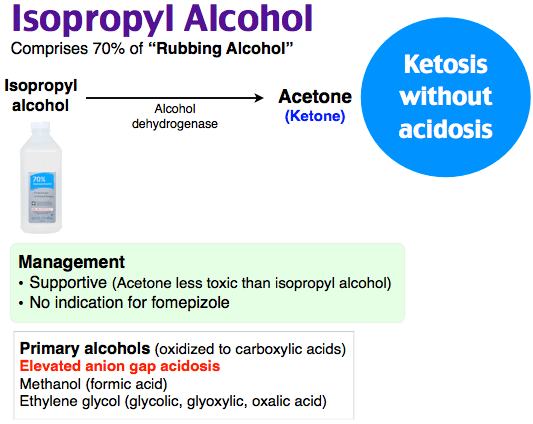
Presentation consistent with isopropyl alcohol intoxication. Isopropyl alcohol is metabolized to acetone (a ketone, not an acid), producing an osmolar gap and ketonemia/ketonuria WITHOUT anion gap metabolic acidosis. This distinguishes it from methanol and ethylene glycol, which produce both an osmolar gap AND an anion gap acidosis. Not consistent with methanol (no acidosis, no visual complaints), ethylene glycol (no acidosis, no renal injury), or ethanol intoxication alone (positive ketones, acetone odor).[1]
Plan: Supportive care and serial reassessments. No antidote needed — fomepizole is not indicated for isopropyl alcohol. IV fluids for dehydration. Monitor for hypotension (isopropyl alcohol is a myocardial depressant and vasodilator). Discharge once improving, ambulating, and tolerating oral intake. Return for recurrent vomiting, confusion, or abdominal pain.
Methanol Poisoning
Patient presents with altered mental status, visual complaints, and metabolic acidosis after suspected methanol ingestion. Labs notable for osmolar gap and anion gap metabolic acidosis.
Methanol itself causes inebriation. Its toxic metabolite, formic acid, causes the anion gap acidosis, retinal toxicity, and basal ganglia necrosis. Visual symptoms (blurred vision, “snowfield” vision, blindness) indicate formic acid accumulation and are an ominous sign. Must differentiate from ethylene glycol (no visual symptoms, renal failure predominates) and other causes of anion gap acidosis.[1]
Plan: Fomepizole 15 mg/kg IV loading dose to block alcohol dehydrogenase and prevent further formic acid production. Poison control consulted. Sodium bicarbonate for acidosis. Folinic acid (leucovorin) 50 mg IV q6h to enhance formate metabolism. Hemodialysis if severe acidosis (pH <7.25), visual symptoms, renal failure, or methanol level >50 mg/dL. Admit to ICU.
Ethylene Glycol Poisoning
Patient presents with altered mental status and metabolic acidosis after suspected ethylene glycol ingestion. Labs notable for osmolar gap and anion gap metabolic acidosis. Concern for progression to renal failure from oxalate crystal deposition.
Ethylene glycol itself causes inebriation. Its toxic metabolites (glycolic acid, oxalic acid) cause the anion gap acidosis and acute renal failure from calcium oxalate crystal deposition in renal tubules. Hypocalcemia from calcium binding to oxalate can cause QT prolongation and tetany. Must differentiate from methanol (visual symptoms predominate, no renal failure) and other causes of anion gap acidosis.[1]
Plan: Fomepizole 15 mg/kg IV loading dose. Poison control consulted. Sodium bicarbonate for acidosis (acidic environment favors oxalate crystal formation, worsening renal injury). Pyridoxine 100 mg IV and thiamine 100 mg IV to shunt metabolism toward less toxic metabolites. Hemodialysis if severe acidosis (pH <7.25), renal failure, or ethylene glycol level >50 mg/dL. Monitor calcium and treat hypocalcemia. Admit to ICU.
Clinical Education
Approach to Toxic Alcohol Ingestion
The key diagnostic question: Is there an osmolar gap, an anion gap, or both? All three toxic alcohols cause an osmolar gap (unmeasured osmoles). Methanol and ethylene glycol also cause an anion gap metabolic acidosis (from toxic metabolites). Isopropyl alcohol causes an osmolar gap WITHOUT acidosis (acetone is a ketone, not an acid).[1]
A normal osmolar gap does not exclude toxic alcohol ingestion. If the toxic alcohol has already been metabolized to its acid metabolite, the osmolar gap falls while the anion gap rises. Early ingestion = high osmolar gap, low anion gap. Late ingestion = low osmolar gap, high anion gap. The two gaps move in opposite directions over time.
Profound acidosis (bicarb <5) in a “drunk” patient should trigger immediate concern for toxic alcohols. Very few conditions produce bicarb this low — primarily toxic alcohols, severe sepsis, and metformin-associated lactic acidosis.
Osmolar Gap and Anion Gap
Osmolar gap = measured serum osmolality − calculated osmolality. Normal is <10. Calculated osmolality = 2(Na) + glucose/18 + BUN/2.8 + ethanol/4.6. An elevated osmolar gap indicates unmeasured osmoles (toxic alcohols, ethanol, mannitol, contrast dye, propylene glycol).[1]
Osmolar gap interpretation pitfalls:
| Scenario | Osmolar Gap | Anion Gap | Interpretation |
| Early ingestion | High | Normal | Parent alcohol present, not yet metabolized |
| Mid-ingestion | High | High | Both parent alcohol and toxic metabolites present |
| Late presentation | Normal | High | Parent alcohol fully metabolized — gap is now all acid |
| Isopropyl alcohol | High | Normal | Acetone is a ketone, not an acid — no acidosis |
Bicarb <10 plus osmolar gap plus negative ethanol level strongly suggests primary toxic alcohol exposure. This combination should prompt immediate treatment with fomepizole while awaiting confirmatory levels.
Isopropyl Alcohol Pearls
Isopropyl alcohol is the most commonly ingested toxic alcohol and the least dangerous of the three. Found in rubbing alcohol, hand sanitizer (though many are now ethanol-based), and windshield washer fluid.[1]
Ketonemia and ketonuria without acidosis is the hallmark. Acetone (the metabolite) is a ketone detected on urine dip and serum ketones, but it is not an acid — so there is no anion gap acidosis. This pattern (positive ketones + no acidosis + osmolar gap) is essentially diagnostic.
Pseudo-renal failure: High acetone levels can cause spurious elevation of serum creatinine on certain lab assays. Be aware of this if nephrology pushes back on a normal creatinine in a patient you believe has renal injury.
Treatment is purely supportive. Fomepizole is not indicated because acetone is not a toxic metabolite. Hemodialysis is only indicated for refractory hypotension or isopropyl alcohol levels >400 mg/dL.
Methanol Pearls
Visual symptoms are the red flag for methanol. Formic acid is selectively toxic to the retina and optic nerve. Patients may describe blurred vision, “snowfield” vision, decreased acuity, or complete blindness. Visual symptoms indicate significant formic acid accumulation and mandate emergent treatment.[2]
Sources: Windshield washer fluid, paint remover, industrial solvents, improperly distilled spirits (moonshine), and de-icing products.
Methanol very often needs hemodialysis. Unlike ethylene glycol (where fomepizole alone may be sufficient in early presentations), methanol has a very long half-life even on fomepizole (~54 hours), and the formic acid metabolite is highly toxic. HD simultaneously removes both the parent alcohol and the toxic metabolite.
Folinic acid (leucovorin) enhances formate metabolism. Give 50 mg IV q6h. If leucovorin is unavailable, folic acid 50 mg IV q6h is a reasonable substitute.
Ethylene Glycol Pearls
Ethylene glycol is found in antifreeze and has a sweet taste, making accidental ingestion (especially pediatric) and intentional ingestion common. The lethal dose is approximately 1.4 mL/kg.[2]
Calcium oxalate crystals in the urine are classic but not sensitive. When present, needle-shaped or envelope-shaped crystals on UA microscopy are highly suggestive. Absence does not exclude the diagnosis.
Hypocalcemia is a unique complication of ethylene glycol. Oxalic acid binds free calcium, causing symptomatic hypocalcemia (tetany, QT prolongation, seizures). Monitor ionized calcium. Replace cautiously — exogenous calcium may worsen oxalate crystal deposition.
Bicarbonate is especially important in ethylene glycol. Acidic pH favors the crystallization of calcium oxalate in renal tubules, accelerating renal injury. Alkalinization with bicarbonate helps prevent crystal deposition in addition to treating the acidosis.
Cofactor therapy: Pyridoxine (B6) 100 mg IV and thiamine (B1) 100 mg IV shunt metabolism of glyoxylic acid toward less toxic metabolites (glycine instead of oxalate).
Fomepizole and Dialysis
Fomepizole is the antidote for methanol and ethylene glycol. It competitively inhibits alcohol dehydrogenase, blocking conversion of the parent alcohol to its toxic metabolites. Loading dose 15 mg/kg IV over 30 minutes, then 10 mg/kg q12h. Dose increases to 15 mg/kg after 48 hours due to autoinduction of its own metabolism.[2]
Fomepizole is NOT indicated for isopropyl alcohol (acetone is not a toxic metabolite).
Ethanol drip is an alternative if fomepizole is unavailable. Target serum ethanol 100-150 mg/dL. Ethanol also competitively inhibits alcohol dehydrogenase but is far harder to titrate, causes additional intoxication, and carries more side effects. Fomepizole is preferred when available.
Hemodialysis indications:
| Indication | Details |
| Severe acidosis | pH <7.25 despite bicarbonate |
| Renal failure | Ethylene glycol with rising creatinine |
| Visual symptoms | Methanol with any visual complaint |
| High levels | Methanol or ethylene glycol >50 mg/dL |
| Clinical deterioration | Worsening despite fomepizole and supportive care |
Important: fomepizole is dialyzed off. Dose fomepizole q4h during dialysis (instead of q12h) to maintain therapeutic levels.
Disposition
Discharge (isopropyl alcohol only): Improving mental status, hemodynamically stable, tolerating oral intake, no significant acidosis. Return for recurrent vomiting, confusion, or abdominal pain.
Admit (ICU): All methanol and ethylene glycol ingestions requiring fomepizole. Any toxic alcohol ingestion with anion gap acidosis. Hemodialysis required. Visual symptoms (methanol). Renal failure (ethylene glycol). Hemodynamic instability.
