pt presents with concern for recent ASA overdose.
Airway maintained.
Unlikely intracranial bleed, ischemic CVA, opioid intoxication, sepsis, hypothyroidism.
Workup: POC glucose, CBC, BMP, LFTs, PT/INR, 4 hour APAP level, salicylate level
ECG: Normal Sinus Rhythm. No overt ischemic findings and no prolongation of QTc or QRS intervals.
Findings: Salicylate level <100mg/mL on 2 consecutive checks over >1 hour
Consults: Will consult psychiatry for potential LPS hold
Exam and findings most consistent with nontoxic level of ASA intoxication without evidence of other ingestion or other emergent medical pathology.
Disposition: Will admit to psychiatry service
PEARLS
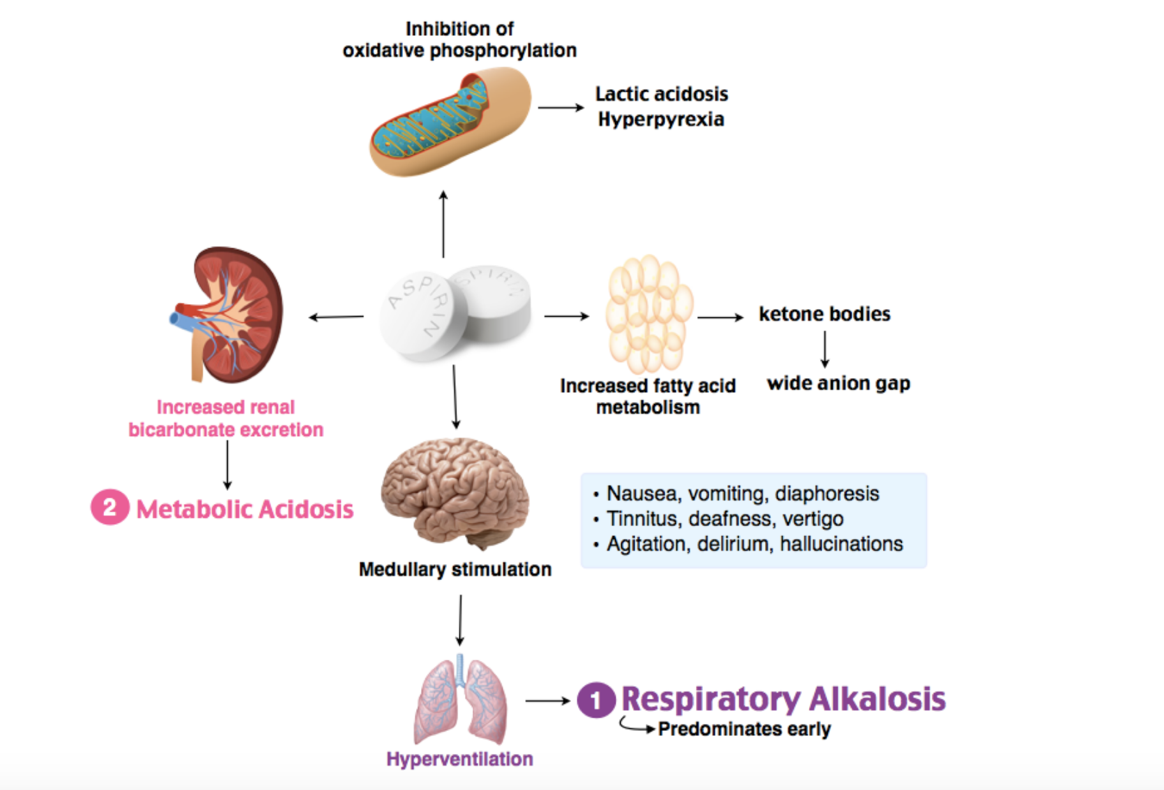
- Clinical presentation
- SOB
- noncardiogenic pulmonary edema (from alteration in the permeability characteristics of the pulmonary capillary membrane)
- Tinnitus
- occurs over level of 30-40 (just before treating with urinary alkalinization)
- SOB
- Tx
- First, fluid deficits and acid-base disturbances must be corrected.
- IVF if no cerebral edema, no pulmonary edema
- Second, excrete toxin through alkalinization of the urine with bicarb.
- Sodium bicarbonate
- NaHCO3 1-2mEq/kg IV bolus; then 3amp bicarb in 1L D5W at 2-3mL/kg/hr. Blood pH goal: 7.5-7.6
- Check K+ because can lead to life-threatening hypokalemia
- “to alkalinize the urine you must keep patients from getting hypokalemic
6.Proudfoot A, Krenzelok E, Vale J. Position Paper on urine alkalinization. J Toxicol Clin Toxicol. 2004;42(1):1-26. https://www.ncbi.nlm.nih.gov/pubmed/15083932.</div> </div>”>6, cause the kidney will preferentially hold on to potassium and dump a proton, preventing the alkalinization. Keep their K > 4.0 meq/L”
- HD indications
- Salicylate toxicity causing noncardiogenic pulmonary edema
- Should also consider intubation
- Intubation with a lung-protective ventilation strategy given likely progression to ARDS
- Low TVs 6-8cc/kg IBW
- Acute toxicity with ASA level > 100 mg/dL and chronic toxicity > 60 mg/dL
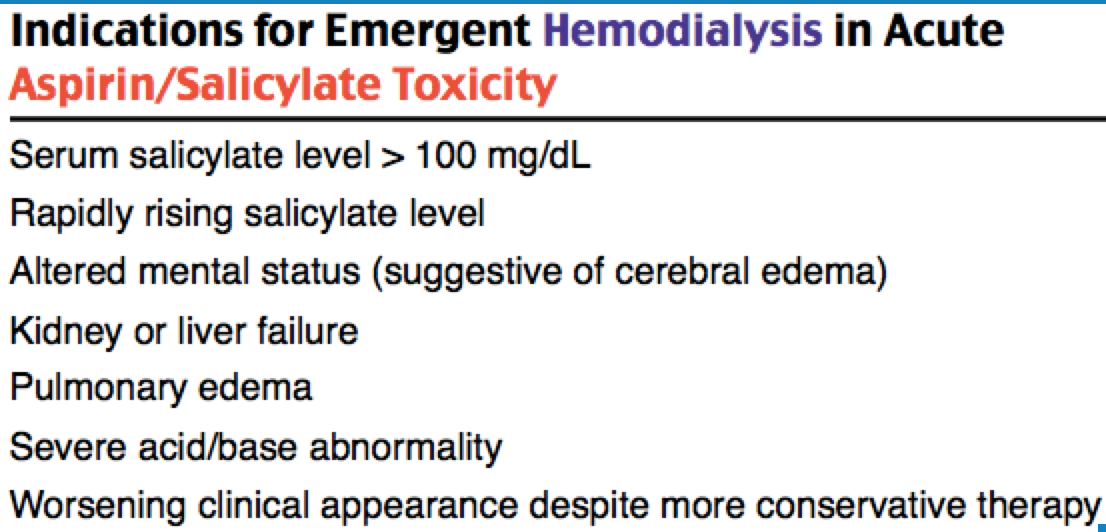
- HD indications
- “to alkalinize the urine you must keep patients from getting hypokalemic
- First, fluid deficits and acid-base disturbances must be corrected.
