Last reviewed: March 2026
Contents
MDM Templates
Tense Ascites / Volume Burden
Patient with known cirrhosis presents with abdominal distension, discomfort, and dyspnea consistent with tense ascites. Well appearing without fever or peritoneal signs. No stigmata of acute hepatic decompensation beyond known baseline.
Therapeutic paracentesis performed (see procedure note). Ascitic fluid sent for cell count with differential, albumin, total protein, and culture. Fluid analysis does not meet criteria for SBP (PMN count < 250 cells/mm³).
Plan: Albumin replacement per volume removed. Diuretic adjustment discussed with patient.
Disposition: Discharge with return precautions for fever, worsening abdominal pain, confusion, or GI bleeding. Follow up with hepatology or PCP within 1 week.
Spontaneous Bacterial Peritonitis
Patient with cirrhosis and ascites presents with abdominal pain and fever. Diagnostic paracentesis performed — ascitic fluid PMN count ≥ 250 cells/mm³, consistent with SBP. Cultures sent.
Plan: Ceftriaxone 2 g IV initiated. IV albumin 1.5 g/kg given on day 1 (with day 3 dose of 1 g/kg to be continued inpatient). Fluid resuscitation as needed.
Disposition: Admit to medicine. Return precautions given for worsening mental status, hematemesis, or hemodynamic instability.
If concern for secondary bacterial peritonitis:
Ascitic fluid analysis raises concern for secondary peritonitis — fluid meets two or more of: total protein > 1 g/dL, glucose upper limit of normal serum. CT abdomen obtained to evaluate for surgical source. Surgery consulted.
New-Onset Ascites
Patient presents with new-onset abdominal distension and exam consistent with ascites in a patient without prior diagnosis of liver disease. Diagnostic paracentesis performed with fluid sent for cell count, albumin, total protein, culture, and cytology given no established etiology.
Plan: Labs sent including hepatic panel, coagulation studies, albumin. Fluid SAAG calculated to guide differential. Patient stable for admission for further workup of new-onset ascites.
Disposition: Admit to medicine for further evaluation.
Procedure Notes
Paracentesis
Indication: Diagnostic and/or therapeutic paracentesis for ascites
Time Out: Correct patient, correct procedure confirmed
Position: Semi-Fowler with slight lateral tilt to dependent side
Ultrasound: Point-of-care ultrasound used to identify a pocket of fluid with adequate depth and absence of underlying bowel. Entry site marked.
Anesthesia: Skin and subcutaneous tissue anesthetized with 1% lidocaine down to the peritoneum
Approach: Area prepped and draped in sterile fashion. 16-gauge blunt-tip needle with trocar inserted using Z-tract technique through the abdominal wall into the peritoneal cavity. Free flow of fluid obtained.
Volume: *** L of serous fluid removed. Fluid sent for cell count with differential, albumin, total protein, culture
Post-procedure: No hypotension. Catheter removed and sterile dressing applied.
Complications: None. Patient tolerated procedure well.
Clinical Education
SBP Pearls
Every cirrhotic patient with ascites who presents to the ED should get a diagnostic paracentesis. SBP can present with fever and abdominal pain, but it can also present with subtle findings — worsening encephalopathy, renal failure, or just “not looking right.” Clinical gestalt alone misses ~30% of SBP cases. The threshold to tap should be extremely low.[1]
PMN count ≥ 250 cells/mm³ = treat for SBP. Don’t wait for cultures — they take 48 hours and are negative in ~40% of culture-negative neutrocytic ascites (which is still SBP and still needs treatment). Initiate antibiotics based on the cell count alone.[1]
Ceftriaxone 2 g IV daily is first-line for community-acquired SBP. For nosocomial SBP or patients with recent fluoroquinolone prophylaxis, consider broader coverage (piperacillin-tazobactam or meropenem) pending cultures.[2]
IV albumin reduces mortality in SBP. The Sort trial demonstrated that albumin 1.5 g/kg on day 1 and 1 g/kg on day 3 reduced renal impairment and mortality from ~29% to ~10%. This is one of the most impactful interventions in SBP management — don’t forget it.[3]
SAAG and Ascitic Fluid Analysis
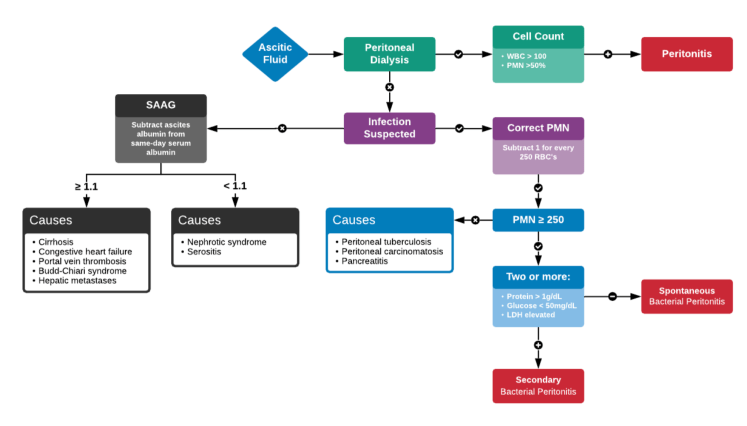
The SAAG (Serum-Ascites Albumin Gradient) is the single most useful test for categorizing ascites. SAAG ≥ 1.1 g/dL indicates portal hypertension (cirrhosis, heart failure, Budd-Chiari). SAAG < 1.1 g/dL suggests peritoneal disease (malignancy, TB peritonitis, nephrotic syndrome). Accuracy is ~97%.[4]
| Test | Always Send | Interpretation |
| Cell count + differential | Yes | PMN ≥ 250 = SBP |
| Albumin | Yes | Needed for SAAG calculation |
| Total protein | Yes | < 1 g/dL = high SBP risk; helps distinguish secondary peritonitis |
| Culture (blood culture bottles) | Yes | Inoculate at bedside for best yield |
| Glucose, LDH | If secondary peritonitis suspected | Glucose < 50, LDH elevated = secondary |
| Cytology | If new-onset ascites | Peritoneal carcinomatosis |
Distinguish SBP from secondary bacterial peritonitis. Secondary peritonitis (perforated viscus, abscess) meets Runyon criteria: ascitic fluid with ≥2 of total protein > 1 g/dL, glucose upper limit of normal for serum. This requires CT and surgical consultation — not just antibiotics.[5]
Paracentesis Pearls
There is no INR or platelet cutoff that contraindicates paracentesis. Cirrhotic coagulopathy does not predict procedural bleeding — these patients have a balanced hemostatic state. Do not transfuse FFP or platelets “to correct the INR” before tapping. This delays care, doesn’t reduce complications, and exposes the patient to unnecessary transfusion risk.[6]
Use the Z-tract technique. Enter the skin one level, then redirect through the abdominal wall at an angle so the skin entry and peritoneal entry don’t align. This prevents post-procedure leaking — a common and annoying complication.
Ultrasound guidance is standard of care. Mark the site with the patient in the same position they’ll be in during the procedure. Left lower quadrant is generally preferred (larger fluid pocket, away from the cecum and right-sided scars from prior surgery).
Albumin Replacement
Give albumin for large-volume paracentesis (>5 L): 6–8 g of albumin per liter removed (typically 25% albumin). This prevents post-paracentesis circulatory dysfunction, which manifests as renal failure and hyponatremia days after the procedure.[7]
For SBP, albumin dosing is separate from volume-based replacement: 1.5 g/kg on day 1 and 1 g/kg on day 3, regardless of paracentesis volume. Both are weight-based, not volume-based.[3]
Hepatorenal Syndrome
Hepatorenal syndrome (HRS) is a diagnosis of exclusion — AKI in a cirrhotic patient that doesn’t respond to volume resuscitation (albumin challenge of 1 g/kg/day for 2 days) and has no other identifiable cause (no nephrotoxins, no shock, no obstruction). Two types: Type 1 (rapid, doubling of creatinine in <2 weeks) is a medical emergency with median survival of 2 weeks without treatment.[8]
In the ED, the key is recognizing that renal failure in a cirrhotic is not always “prerenal from poor intake.” If creatinine doesn’t improve with albumin resuscitation and there’s no other explanation, suspect HRS and involve hepatology early. Treatment is terlipressin + albumin (or midodrine + octreotide + albumin where terlipressin is unavailable).
Disposition
Admit if: SBP (PMN ≥ 250), new-onset ascites requiring workup, hepatorenal syndrome, hepatic encephalopathy, concomitant GI bleed, or hemodynamic instability.
Discharge if: Known cirrhosis with tense ascites after therapeutic paracentesis, ascitic fluid without evidence of SBP, tolerating PO, hemodynamically stable, reliable follow-up. Ensure albumin replacement is given before discharge if large-volume paracentesis performed.
References
- Runyon BA. AASLD Practice Guideline: Management of adult patients with ascites due to cirrhosis — update 2012. Hepatology. 2013;57(4):1651-1653. PubMed
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol. 2010;53(3):397-417. PubMed
- Sort P et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med. 1999;341(6):403-409. PubMed
- Runyon BA et al. The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites. Ann Intern Med. 1992;117(3):215-220. PubMed
- Runyon BA, Hoefs JC. Ascitic fluid analysis in the differentiation of spontaneous bacterial peritonitis from gastrointestinal tract perforation into ascitic fluid. Hepatology. 1984;4(3):447-450. PubMed
- Grabau CM et al. Performance standards for therapeutic abdominal paracentesis. Hepatology. 2004;40(2):484-488. PubMed
- Bernardi M et al. Albumin infusion in patients undergoing large-volume paracentesis: a meta-analysis of randomized trials. Hepatology. 2012;55(4):1172-1181. PubMed
- Angeli P et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. J Hepatol. 2015;62(4):968-974. PubMed
