MDM Templates
Elbow Fracture
Patient presents with elbow pain after injury. Imaging demonstrates fracture. They do not currently demonstrate complications such as compartment syndrome, neurovascular injury, or open fracture. The fracture has been satisfactorily immobilized.
History and exam not consistent with compartment syndrome, arterial or nerve injury. Motor exam intact — elbow extension against resistance intact, finger abduction and adduction intact, wrist extension intact. Sensation intact distally.
Plan: Posterior splint and sling. Analgesics.
Disposition: Discharge with return precautions for worsening pain, numbness, swelling, or inability to move fingers. Orthopedic follow-up within 1 week.
Radial Head Fracture
Patient presents with lateral elbow pain after fall on outstretched hand. Imaging demonstrates radial head fracture. Exam with focal tenderness over radial head, pain with forearm pronation/supination. Full extension intact. No mechanical block to motion. Neurovascular exam intact distally.
History and exam not consistent with elbow dislocation, coronoid fracture, or terrible triad injury. No mechanical block suggesting loose body.
Plan: Sling for comfort. Analgesics. Early gentle range of motion as tolerated.
Disposition: Discharge with orthopedic follow-up within 1 week.
Elbow Dislocation
Patient presents with elbow deformity and inability to move the affected extremity after injury. Imaging confirms posterior elbow dislocation. Neurovascular exam intact distally prior to reduction.
Dislocation reduced at bedside under procedural sedation. Post-reduction imaging confirms anatomic reduction without associated fracture. Neurovascular status intact before and after reduction. Elbow stable through range of motion testing.
Plan: Posterior splint at 90 degrees of flexion. Analgesics.
Disposition: Discharge with orthopedic follow-up within 1 week. Return precautions for worsening pain, numbness, or swelling.
If fracture-dislocation (terrible triad):
Orthopedics consulted regarding fracture pattern, joint stability, and need for operative fixation. Immobilized in long arm posterior splint with forearm in supination.
Olecranon Bursitis
Patient presents with swelling over the posterior elbow at the olecranon. Exam consistent with olecranon bursitis — fluctuant swelling without joint effusion, full range of motion of the elbow, no erythema or warmth suggesting septic bursitis. Well appearing without fever.
History and exam lower suspicion for elbow fracture, dislocation, septic bursitis, and compartment syndrome.
Plan: Compression wrap, ice, NSAID. Aspiration deferred given non-infectious appearance.
Disposition: Discharge with return precautions for fever, spreading redness, or worsening pain. Follow up with PCP within 1 week.
If concern for septic bursitis (erythema, warmth, fever): Aspiration performed — fluid sent for cell count, gram stain, culture, and crystal analysis. Empiric antibiotics started pending culture results.
Upper Extremity Tendon Injury
Patient presents with pain and weakness after injury to the upper extremity. Exam demonstrates loss of function consistent with tendon injury. Neurovascular exam intact distally. No signs of compartment syndrome.
History and exam not consistent with fracture, dislocation, neurovascular injury, or compartment syndrome. Presentation consistent with tendon injury requiring outpatient surgical evaluation.
Plan: Sling immobilization. Analgesics.
Disposition: Discharge with orthopedic follow-up within 1 week. Patient understands that ED care is stabilizing and that operative repair may be required.
Clinical Education
Supracondylar Fracture Pearls
This is the most common elbow fracture in children and the one most likely to have vascular complications. The anterior interosseous nerve (AIN) is the most commonly injured nerve — test with “OK sign” (thumb-index finger pinch). The brachial artery can be trapped or kinked. Always check radial pulse and capillary refill before and after any manipulation.[1]
| Finding | Management |
| Occult (fat pads only) or non-displaced | Long arm posterior splint at 45–90 degrees, ortho follow-up |
| Any cortical separation (Gartland type II+) | Consult ortho — closed reduction with percutaneous pinning (can wait until morning unless poor perfusion) |
| Pulseless extremity | Emergent ortho consult — attempt gentle reduction, reassess pulse |
Olecranon Fracture Pearls
Test the extensor mechanism — can the patient extend the elbow against gravity? Loss of active extension indicates disruption of the triceps mechanism through the fracture, which typically needs operative fixation. Non-displaced fractures (<2 mm) with intact extensor mechanism can be managed conservatively with posterior splint and early motion at 2–3 weeks. Immobilization beyond 3 weeks risks chronic elbow stiffness.[2]
Check the ulnar nerve. It runs in the cubital tunnel just medial to the olecranon and can be injured with olecranon fractures. Test small finger tip sensation and finger abduction strength.
Radial Head Fracture Pearls
The radial head is the most commonly fractured bone in the adult elbow. FOOSH (fall on outstretched hand) drives force through the lateral elbow due to the normal valgus carrying angle. Most are non-displaced and managed with a sling and early motion — prolonged immobilization does more harm than good.[3]
Consult ortho for: >30 degrees angulation, >3 mm displacement, >33% of radial head surface involved, or any mechanical block to forearm rotation (suggests loose body in the joint).
Radial head fracture on lateral view
The Terrible Triad
Radial head fracture + coronoid fracture + elbow dislocation = terrible triad. This combination creates a grossly unstable joint. The coronoid fracture can be subtle on X-ray — look carefully on the lateral view. If you see a radial head fracture with an elbow dislocation, assume a coronoid fracture exists until proven otherwise. Immobilize in a long arm posterior splint with the forearm in supination and consult orthopedics — these almost always need surgery.[4]
Elbow Dislocation Pearls
Reduction technique: Two common approaches work well. Option 1: With the patient supine, flex the elbow while applying longitudinal traction on the forearm and direct pressure over the olecranon anteriorly. Option 2: Prone with arm hanging off the bed — one provider pulls downward traction on the hand while another lifts the bicep and pushes the olecranon anteriorly with their thumbs.[5]
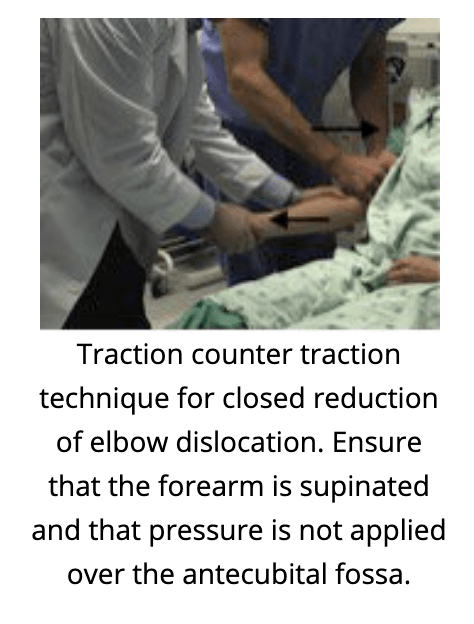
Elbow reduction technique
Post-reduction expectations to set at discharge: Likely unable to fully extend beyond 30 degrees for ~6 weeks. Full extension at 2–3 months. Weight-bearing exercises at ~4 months. Simple dislocations (no fracture) need ❤ weeks of immobilization — longer leads to stiffness. Fracture-dislocations need ortho within 72 hours for ORIF evaluation.
Biceps and Triceps Tendon Injury
Distal biceps rupture is the one that needs urgent surgery. Test with the hook test — try to hook your finger under the biceps tendon in the antecubital fossa. If you can’t feel the tendon, it’s ruptured. Also test supination strength (Jergesen’s test — resist doorknob-turning motion) — patients may have preserved flexion from the brachialis but weak supination. Distal ruptures need operative repair within 2–3 weeks before the muscle retracts and the tendon becomes irretrievable.[6]
Proximal biceps rupture is less urgent. These present with a “Popeye deformity” — the muscle belly bunches distally. Managed with sling, PT, and outpatient ortho follow-up. Most do well without surgery.
Triceps tendon rupture is rare. Look for a palpable divot posterior to the olecranon and inability to extend the elbow against gravity. Sling and ortho follow-up within 1–2 weeks — operative repair typically needed within 6 weeks.
Imaging note: Ultrasound frequently misses partial tendon injuries. These are primarily clinical diagnoses.
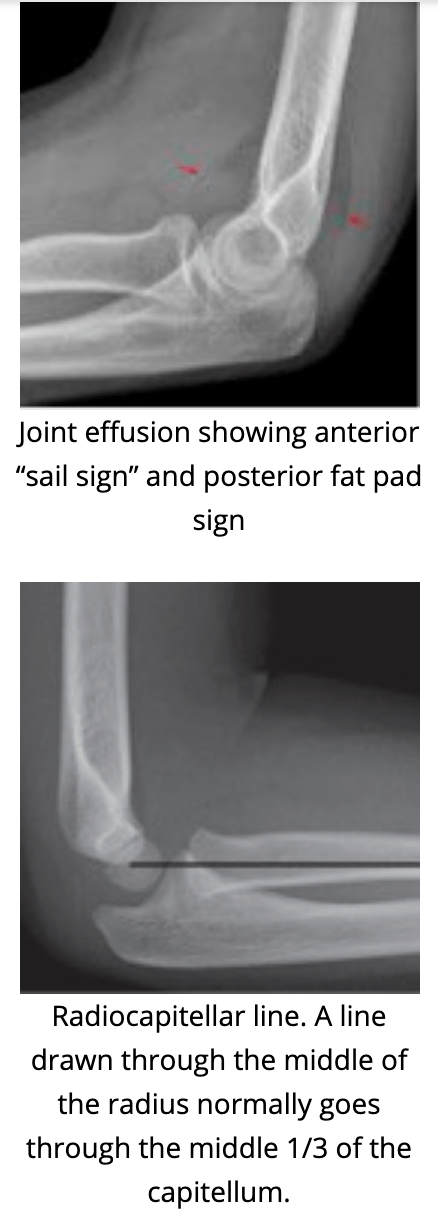
Fat Pad Sign
A posterior fat pad on a lateral elbow X-ray indicates an intra-articular fracture until proven otherwise. The posterior fat pad is normally hidden in the olecranon fossa — it only becomes visible when pushed out by a joint effusion (blood). An anterior “sail sign” (elevated anterior fat pad) is less specific but also suggests effusion. If you see fat pads but no obvious fracture line, treat as an occult fracture — splint and arrange ortho follow-up. In children, this means a supracondylar fracture; in adults, think radial head fracture.[7]
References
- Omid R et al. Supracondylar humeral fractures in children. J Bone Joint Surg Am. 2008;90(5):1121-1132. PubMed
- Duckworth AD et al. The epidemiology of fractures of the proximal ulna. Injury. 2012;43(3):343-346. PubMed
- Duckworth AD et al. Radial head and neck fractures: functional results and predictors of outcome. J Trauma. 2011;71(3):643-648. PubMed
- Pugh DM et al. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am. 2004;86(6):1122-1130. PubMed
- Mehlhoff TL et al. Simple dislocation of the elbow in the adult. J Bone Joint Surg Am. 1988;70(2):244-249. PubMed
- O’Driscoll SW et al. The hook test for distal biceps tendon avulsion. Am J Sports Med. 2007;35(11):1865-1869. PubMed
- Skaggs DL, Mirzayan R. The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am. 1999;81(10):1429-1433. PubMed
