Last reviewed: March 2026
Contents
MDM Templates
Esophageal Food Bolus
Patient presents with acute onset dysphagia and globus sensation after eating, consistent with esophageal food impaction. Able to manage secretions. No stridor, respiratory distress, or signs of airway compromise. No chest pain, subcutaneous emphysema, or signs of esophageal perforation.
If tolerating secretions and stable:
Trial of conservative management with carbonated beverage and observation. Patient demonstrates passage of bolus with ability to tolerate liquids and solids orally.
Disposition: Discharge with follow-up for outpatient EGD to evaluate for underlying esophageal pathology (eosinophilic esophagitis, stricture, Schatzki ring). Return for recurrent dysphagia, chest pain, or inability to tolerate secretions.
If unable to pass bolus after conservative trial:
Food impaction persistent after conservative management. GI consulted for endoscopic removal. No signs of perforation or complete obstruction.
Disposition: Admit for EGD. Food bolus should not remain in the esophagus beyond 12 hours due to risk of mucosal injury.
Esophageal Foreign Body — Non-Food
Patient presents after ingestion of a foreign object currently lodged in the esophagus on imaging. Hemodynamically stable. No signs of airway compromise or perforation.
GI consulted for endoscopic removal. Object characteristics: ***.
Disposition: Admit for endoscopic removal. Emergent EGD if sharp, pointed, or causing complete obstruction.
Button Battery Ingestion
Patient (child / adult) presents after ingestion of a button battery. Imaging demonstrates battery location in the ***.
If in esophagus:
Button battery lodged in esophagus — this is a time-critical emergency. Esophageal necrosis and perforation can occur within 2 hours. GI and surgery consulted emergently for immediate endoscopic removal. Patient made NPO. National Button Battery Ingestion Hotline contacted (202-625-3333). If honey is available and patient is over 12 months, honey 10 mL every 10 minutes given while awaiting endoscopy per NBIH protocol.
If beyond esophagus:
Button battery confirmed beyond the esophagus on imaging. No signs of obstruction or perforation. Expected to pass spontaneously in most cases.
Disposition: Discharge with instructions to monitor stools for passage. Return for abdominal pain, vomiting, bloody stool, or if battery has not passed in 48 hours. Follow-up X-ray if not passed.
Distal GI Foreign Body
Patient presents after ingestion of a foreign body. Imaging confirms the object is beyond the esophagus in the ***. Object is blunt, small (< 2 cm wide, < 6 cm long), and without sharp edges. No signs of obstruction or perforation.
Object expected to pass spontaneously without intervention. No indication for whole bowel irrigation or endoscopic retrieval at this time.
Disposition: Discharge with instructions to monitor stools for passage. Return for abdominal pain, vomiting, bloody stool, or fever. Follow-up X-ray if not passed in 1 week.
Body Packing / Body Stuffing
Patient presents with concern for ingestion of drug-containing packets. Hemodynamically stable. No signs of drug toxicity at this time. Imaging demonstrates ***.
Plan: Whole bowel irrigation with polyethylene glycol electrolyte solution initiated. Serial abdominal exams. Continuous cardiac monitoring. Surgery and toxicology consulted.
Disposition: Admit for observation and monitored passage. Surgical intervention if signs of obstruction, packet rupture, or drug toxicity develop.
Clinical Education
When to Call Emergent EGD
Emergent endoscopy (within 2 hours) is indicated for:[1]
| Indication | Rationale |
| Button battery in esophagus | Perforation within 2 hours |
| Complete esophageal obstruction (can’t manage secretions) | Aspiration risk |
| Sharp/pointed object in esophagus | Perforation risk up to 35% |
| Multiple magnets in esophagus or stomach | Can attract across bowel walls → necrosis |
Urgent endoscopy (within 24 hours): Esophageal food bolus not clearing with conservative measures, esophageal coins in children, objects > 2 cm wide or > 6 cm long in the stomach (unlikely to pass pylorus).
Food Bolus Management
Carbonated beverages are reasonable first-line. The CO₂ distends the esophagus and may help the bolus pass. Success rate is modest (~60% in some series) but the intervention is safe and buys time.[2]
Glucagon 1 mg IV is widely used but poorly supported by evidence. Multiple studies show no significant benefit over placebo. It can cause vomiting (dangerous with a foreign body in the esophagus). Some GI consultants still prefer it — use it per your consultant’s preference, but don’t delay endoscopy waiting for it to work.[3]
Don’t leave a food bolus in the esophagus for more than 12 hours. Prolonged impaction causes mucosal edema, ulceration, and increases perforation risk during subsequent endoscopic removal.
Most food impactions have an underlying cause. Eosinophilic esophagitis is the most common etiology in young adults. Schatzki ring and peptic stricture are common in older adults. All patients with food impaction should be referred for outpatient EGD to identify and treat the underlying pathology.[1]
Button Battery Pearls
Button batteries in the esophagus are a true emergency. The battery generates a current against the esophageal mucosa, creating a hydroxide-rich alkaline environment that causes liquefactive necrosis. Perforation can occur within 2 hours. Fistulas to the aorta (fatal aortoesophageal fistula) have been reported even days after removal.[4]
Honey (10 mL q10min) is now recommended while awaiting endoscopy for esophageal batteries in children > 12 months. Honey is viscous and mildly acidic, which neutralizes the alkaline injury and coats the mucosa. Sucralfate is an alternative. Do not use in children < 12 months (botulism risk).[4]
National Button Battery Ingestion Hotline: 202-625-3333. Available 24/7 for guidance on management.
Batteries beyond the esophagus usually pass without issue. The exception: if the child is symptomatic (abdominal pain, vomiting, bloody stools) or the battery hasn’t passed in 48 hours, repeat imaging and consider endoscopic or surgical retrieval.
Magnet Ingestion
A single magnet is generally safe — treat like any other small blunt object and expect spontaneous passage. Multiple magnets (or a magnet + metallic object) are dangerous. They can attract across adjacent bowel loops, causing pressure necrosis, perforation, fistula, or volvulus. These require emergent removal if accessible endoscopically, or surgical consultation if beyond endoscopic reach.[5]
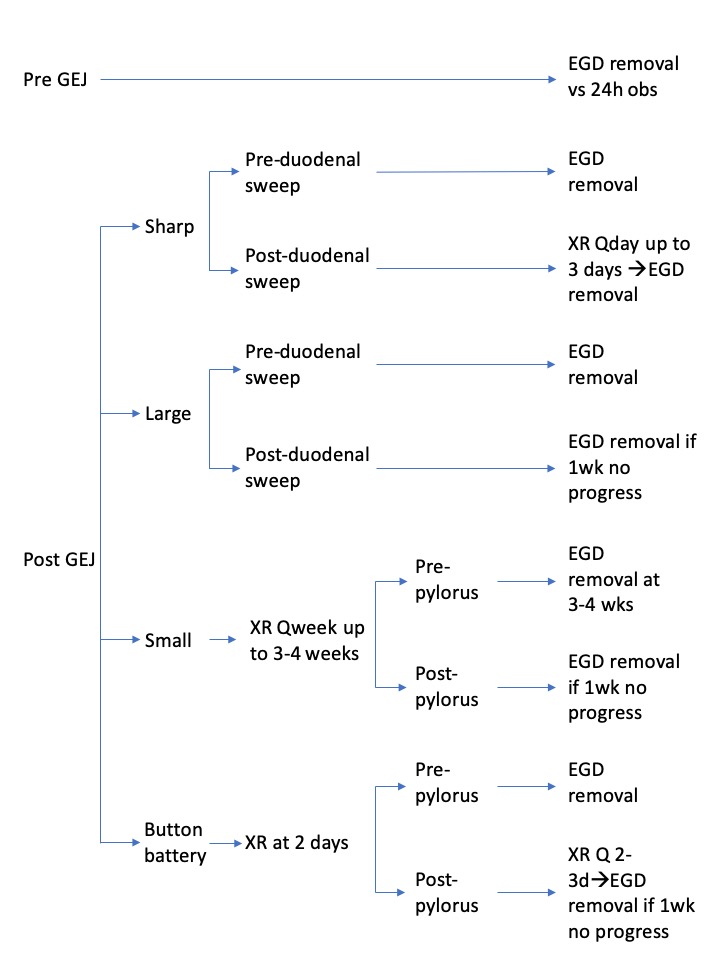
Sharp and Elongated Objects
Sharp objects in the esophagus need emergent removal. Once past the pylorus, sharp objects still carry ~15–35% perforation risk. Daily X-rays to monitor progression. If the object fails to advance over 3 days, or if the patient develops peritoneal signs, surgical intervention is indicated.[1]
Objects > 6 cm long or > 2 cm wide are unlikely to pass the pylorus or duodenal sweep. These should be removed endoscopically from the stomach before they advance into more difficult-to-reach territory.
Do NOT give whole bowel irrigation or cathartics for sharp objects. Accelerated transit increases the risk of perforation.
Body Packing Pearls
Body packers (“mules”) swallow professionally wrapped drug packets for transport. Body stuffers hastily swallow loosely wrapped drugs to avoid arrest. Stuffers are at higher risk for acute toxicity because their packaging is less reliable.[6]
CT abdomen is the best imaging modality — sensitivity ~95% for body packing. Plain X-ray can miss packets. Look for multiple well-defined round or oval densities (“double condom sign”).
Whole bowel irrigation (GoLYTELY 2 L/hr via NGT) is the treatment — continue until rectal effluent is clear and repeat imaging confirms passage. Surgery is reserved for obstruction, packet rupture, or failure to progress. Never attempt endoscopic removal — the risk of packet rupture is too high.
If packet rupture is suspected (acute drug toxicity): For cocaine packets, supportive care with benzodiazepines — do not use beta-blockers. For heroin/opioid packets, naloxone drip. Emergent surgical removal (laparotomy) is indicated.
References
- Birk M et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: ESGE Clinical Guideline. Endoscopy. 2016;48(5):489-496. PubMed
- Karanjia ND, Rees M. The use of Coca-Cola in the management of bolus obstruction in benign oesophageal stricture. Ann R Coll Surg Engl. 1993;75(2):94-95. PubMed
- Leopard D et al. Systematic review of the use of glucagon in the management of oesophageal food bolus impaction. Emerg Med J. 2011;28(5):401-404. PubMed
- Anfang RR et al. pH-neutralizing esophageal irrigations as a novel mitigation strategy for button battery injury. Laryngoscope. 2019;129(1):49-57. PubMed
- Kramer RE et al. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr. 2015;60(4):562-574. PubMed
- Traub SJ et al. Body packing — the internal concealment of illicit drugs. N Engl J Med. 2003;349(26):2519-2526. PubMed
