Last reviewed: March 2026Contents
MDM Templates
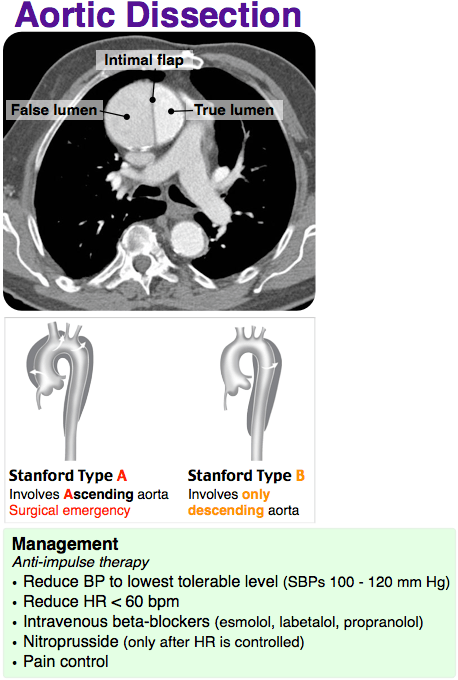
Aortic Dissection
Patient with acute aortic dissection identified on CTA.
Stanford Type: *** (ascending / descending).
No signs of tamponade, malperfusion syndrome, or aortic rupture at this time.
No evidence for concomitant ACS, pulmonary embolism, pneumothorax, and tension pneumothorax as alternative etiologies for this presentation.
Anti-impulse therapy initiated:
Rate control (goal HR 60-80): Esmolol 0.5mg/kg IV bolus over 1min, then gtt at 0.05mg/kg/min titrated to goal.
Pressure control (goal SBP 100-120): Nicardipine 5mg/hr, titrated up by 2.5mg/hr q10min to goal.
Analgesia: Fentanyl 50mcg IV PRN (pain drives sympathetic surge — aggressive analgesia is therapeutic).
Consults: Cardiothoracic / vascular surgery notified.
Disposition: Admit to ICU for continued anti-impulse therapy and surgical planning.
Type A (ascending): Emergent surgical repair — OR notification and blood bank crossmatch initiated.[1]
Type B (descending), uncomplicated: Medical management with anti-impulse therapy. Surgical/endovascular intervention reserved for complicated Type B (malperfusion, rupture, refractory pain, rapid aortic expansion).[1]
Critical Care Time
Given the high probability of imminent or life-threatening deterioration, the patient was immediately assessed and cardiac monitoring initiated with continuous pulse oximetry and supplemental oxygen.
During the course of the patient’s stay, I spent considerable time at the bedside performing serial re-evaluations of hemodynamic and clinical status given the recognized threat to life. Clinical management involved high-complexity decision making to assess, manipulate, and support vital organ system function. All available laboratory and radiographic studies were reviewed along with available prior records. Sequential vital signs were obtained.
Critical care time noted below was time spent engaged in work directly related to this individual patient’s care, not including time performing separately billable procedures.
Total critical care time elapsed: *** minutes.
Body system at highest risk: Cardiovascular.
Clinical Education
Stanford Classification
| Type | Anatomy | Management | Mortality |
| A | Involves ascending aorta (regardless of origin) | Emergent surgical repair + anti-impulse therapy | ~1-2% per hour untreated; ~25% surgical mortality[1] |
| B | Descending aorta only (distal to L subclavian) | Medical management unless complicated (malperfusion, rupture, refractory pain) | ~10% in-hospital with medical management[1] |
DeBakey classification is older but still referenced: Type I (ascending + descending), Type II (ascending only), Type III (descending only). Stanford is more useful for ED decision-making because it drives the surgical vs medical management question.
Anti-Impulse Therapy
Beta-blocker FIRST, then vasodilator. Starting a vasodilator (nicardipine, nitroprusside) before adequate beta-blockade causes reflex tachycardia — increased dP/dt (aortic wall shear stress) worsens dissection propagation. Always get the heart rate down before dropping the pressure.[2]
| Agent | Dose | Pearl |
| Rate control (goal HR 60-80) — start first | ||
| Esmolol | 0.5mg/kg bolus, gtt 0.05-0.2mg/kg/min | Short half-life (~9min) — best if worried about tolerability. Easy to titrate off |
| Labetalol | 20mg IV, then 20-80mg q10min (max 300mg); gtt 1-2mg/min | Alpha + beta blockade — reduces HR and BP simultaneously. Longer half-life |
| Diltiazem | 0.25mg/kg IV, gtt 5-15mg/hr | If BB contraindicated (severe asthma/COPD). Consider if aortic regurgitation murmur present[2] |
| Pressure control (goal SBP 100-120) — add after HR at goal | ||
| Nicardipine | 5mg/hr, titrate by 2.5mg/hr q10min (max 15mg/hr) | First-line vasodilator. Once at goal, decrease to 3mg/hr and re-titrate from there |
| Clevidipine | 1-2mg/hr, titrate by doubling q90sec (max 32mg/hr) | Ultra-short acting. Lipid emulsion — contraindicated in egg/soy allergy |
Analgesia matters: Fentanyl 25-100mcg IV PRN is first-line. Pain drives sympathetic surge → increased HR and BP → worsens dissection. Aggressive pain control is not just comfort — it’s therapeutic.[2]
Malperfusion Syndromes
The dissection flap can obstruct branch vessels at any level. Malperfusion converts uncomplicated Type B to complicated (surgical indication) and worsens Type A mortality.[3]
| Territory | Vessel | Presentation |
| Cerebral | Carotid / vertebral | Stroke, AMS — do NOT give tPA |
| Coronary | Usually RCA (right coronary ostium) | Inferior STEMI pattern — do NOT go to cath lab |
| Spinal | Artery of Adamkiewicz | Paraplegia / paraparesis |
| Mesenteric | SMA / celiac | Abdominal pain out of proportion, lactic acidosis |
| Renal | Renal artery | AKI, flank pain, hematuria |
| Limb | Iliac / femoral | Acute limb ischemia, pulse deficit |
Deadly mimics: Dissection presenting as stroke gets tPA → hemorrhagic catastrophe. Dissection presenting as inferior STEMI gets heparin + cath lab → aortic rupture. Always think dissection before thrombolytics or anticoagulation in chest/back pain with neurologic or vascular findings.[3]
ADD-RS & D-Dimer Rule-Out
The Aortic Dissection Detection Risk Score (ADD-RS) combined with D-dimer can be used to rule out aortic dissection in low-risk patients, avoiding CTA.[4]
ADD-RS ≤1 + D-dimer <500 ng/mL → dissection effectively ruled out (sensitivity 98.8-100% in validation studies). This pathway is now supported by the 2022 ACC/AHA Aortic Disease Guideline as a Class IIa recommendation.[5]
ADD-RS components (1 point per category present):
| Category | Features (any = 1 point) |
| High-risk conditions | Marfan, connective tissue disease, FHx aortic disease, known aortic valve disease, known aortic aneurysm, prior aortic manipulation/surgery |
| High-risk pain features | Chest/back/abdominal pain that is abrupt onset, severe intensity, or described as ripping/tearing |
| High-risk exam findings | Pulse deficit or BP differential, new aortic regurgitation murmur, hypotension/shock, focal neurological deficit + pain |
If ADD-RS ≥2 or D-dimer ≥500 → proceed to CTA aortogram. Do not use this pathway to rule out dissection in patients where your clinical suspicion is already high.
Complications
Cardiac tamponade: Type A dissection can rupture into the pericardium. Presents with Beck’s triad (hypotension, JVD, muffled heart sounds) or PEA arrest. Bedside echo shows pericardial effusion. Emergent pericardiocentesis is a bridge — definitive treatment is OR. Do NOT give large-volume fluid resuscitation (worsens tamponade physiology with permissive hypotension).[1]
Acute aortic regurgitation: Type A dissection can disrupt the aortic valve. New diastolic murmur + acute pulmonary edema. Medical management is a temporizing measure — emergent surgical valve repair/replacement needed.
Aortic rupture: Free rupture into mediastinum, pleural space, or peritoneum. Usually rapidly fatal. Left hemothorax on CXR in setting of acute dissection is ominous.
Exam & Presentation Pearls
Chest pain + new neurologic deficit = dissection until proven otherwise. Example: L common carotid dissection flap → L MCA hypoperfusion → right-sided hemiparesis and facial droop. This patient will look like a stroke — and getting it wrong is lethal.[3]
Blood pressure differentials: Check BP in both arms. >20mmHg systolic difference is concerning. Consider right radial arterial line for monitoring — the innominate artery is the first branch off the arch, so the right arm pressure is most likely to reflect true central aortic pressure unless that vessel is compromised.
CXR clues: Widened mediastinum (>8cm), abnormal aortic contour, left pleural effusion, tracheal deviation. But a normal CXR does NOT rule out dissection — sensitivity is only ~60-90%.[6]
Workup: ECG (rule out STEMI — but remember dissection can cause STEMI), troponin, CBC, BMP, type and crossmatch, lactate (malperfusion), CTA aortogram (chest/abdomen/pelvis with arterial-phase gating for best sensitivity). See also: Radiopaedia: Aortic Dissection.
References
- Isselbacher EM et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. Circulation. 2022;146(24):e334-e482. PubMed
- Hiratzka LF et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease. Circulation. 2010;121(13):e266-e369. PubMed
- Bossone E, Eagle KA. Epidemiology and Management of Aortic Disease: Aortic Aneurysms and Acute Aortic Syndromes. Nat Rev Cardiol. 2021;18(5):331-348. PubMed
- Nazerian P et al. Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes (ADvISED). Circulation. 2018;137(3):250-258. PubMed
- Defined in ref-1: 2022 ACC/AHA Aortic Disease Guideline — Class IIa recommendation for ADD-RS + D-dimer rule-out pathway.
- von Kodolitsch Y et al. Chest Radiography for the Diagnosis of Acute Aortic Syndrome. Am J Med. 2004;116(2):73-77. PubMed
